


The First Myeloma Patient

As late as 1998, myeloma research and treatment were anything but popular in professional circles, much less so in public awareness. Indeed, many myeloma patients then weren’t much better off than the first known patient with the disease.
Sarah Newbury experienced back pains severe enough to seek out Dr. Samuel Solly, a physician in 1840 London. Dr. Solly “found her sitting up in bed, her countenance very cheerful, and excepting its extreme emaciation, not unhealthy.”
To demonstrate what a distance of more than 190 years might make, I doubt that today, many physicians would use the terms “extreme emaciation” and “not unhealthy” in the same sentence. Solly was an optimist, but optimism alone couldn’t change reality.
As her husband carried her to the warmth of a fireplace during a cold day two years later, what little weight she had pressed down and broke the brittle thigh bones resting on his arms. Two years later, Newbury’s decline led to her admission to a hospital in 1844. After being treated with orange peel, rhubarb pills, and “fortunately with opiates,” she would die five days later.
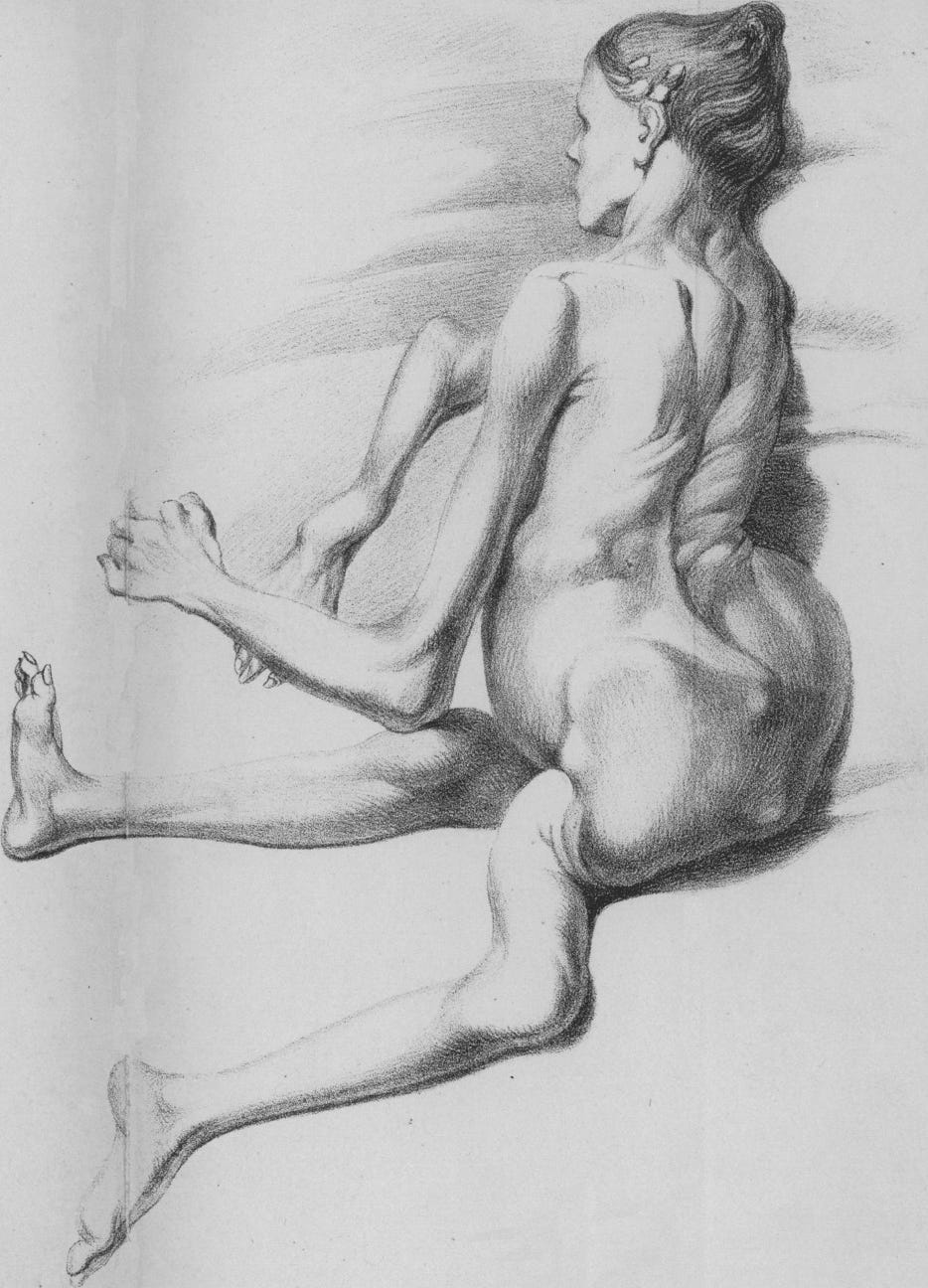
Newbury’s case was so bad, an untrained eye could look at Solly’s drawing of her and be immediately horrified. Broken limbs splayed at unnatural angles and compressed, collapsing each bone in her spine slowly, causing her chin to curl down toward her sternum, changing the pitch of her voice.
Newbury’s agony lasted four years, which, frustratingly correlated to the average survival after diagnosis patients still would experience more than 150 years later. And four years was far longer than the norm. Making it more mysteriously menacing, virtually every diagnosed patient never heard the word myeloma until they were told they had it.
By the end of the 20th century, most knew melanoma was on the skin, but where was myeloma? And what was it? Bones ached, sudden fracturing or breaking — ribs from coughing or leg bones from making a normal step up or down — were relatively common individual horror stories shared by patients that had so much in common in others with the same diagnosis.
Although the pain, discomfort, symptoms, side effects, and every other piece of baggage that came with the disease could be scientifically explained, the totality of it was something that had to be personally experienced to truly grasp. Even experienced treating experts would never really know what their patients felt like inside unless they were patients themselves, but they could explain it in theory with exceptional detail and insight.
Myeloma cells are plasma cells that become cancerous, or malignant. Plasma cells, making up just one percent of healthy bone marrow, are essential to create blood and maintain immune systems. Plasma and myeloma are over-achievers with differing intentions. No one really notices plasma when it works as advertised. But it seems myeloma has a biological signal, to tell plasma it is the new boss and take charge. Myeloma cells “crowd out” healthy cells in the marrow.
Rather than the normal one percent of plasma cells in the marrow, they proliferate to become 70-80-90%, essentially destructive killers, preventing normal functions of physiological systems. Consequences can be deadly, upsetting the normal balance bone destruction and rebuilding occurring naturally and continually in every healthy person, even as it slows down naturally during the aging process.
The cell responsible for degrading old bone tissue, the osteoclast, becomes turbo-charged, destroying more bone. The bone-rebuilding cell, the osteoblast, takes “a vacation,” or at the very least, is prevented from doing its job, the most visible sign being bone lesions, hole-like thinning that increases the risk of fractures.
It explained why initial descriptions of the disease were associated with bone softening: or mollities ossium, as they were called in the medical literature of the time. And this explained why, for more than 150 years, many patients in advanced stages could lose inches of height due to collapsing vertebrae.
Patients could also expect persistent sluggishness due to anemia, which inhibited growth of red bloods cells which are essential to deliver oxygen throughout the body. Loosened calcium from bones would settle in kidneys, caused by all sorts of problems as they progressed toward complete failure. Simple infections like bug bites or scratches could send a compromised immune system into a tailspin, often leading to potentially deadly complications.
Common colds, a normal nuisance for most, became deadly minefields for myeloma patients. Many patients were diagnosed with no symptoms, usually because of something seen in a routine blood test. Plus, the prospect of chemotherapy came with an expectation to which any cancer patient could relate; life would be more miserable before it hopefully got better.
The many routes taken to treat a myeloma patient had not translated into much of anything positive for patients as the 20th century neared its end. Thousands of patients could still intimately describe the pain of collapsed vertebrae causing downward and inward collapsing of the chin toward the chest that Sarah Newbury experienced in 1844. The few doctors who were aware of her case could only describe symptoms. They had no idea what caused them.
It would take years before some would begin to figure it out. Keep checking in on this Substack to learn more about the people and ideas that made remarkable progress in myeloma possible.
Photo: Detail from sketch of Sarah Newbury, Solly, Samuel, Remarks on the Pathology of Mollities Ossium. With Cases. (1844).
Thank you! Really appreciate it. Have some interesting stories to be posted in next few weeks!
I am so glad you are publishing on Substack and great job on your research and writing. You are bringing much light and hope for myeloma patients, like me! I’ll share in all my online groups.